In endodontics, referred cases often present significant challenges that test both clinical decision-making and technical precision. This Advanced Case comes from Dr. Othman H. Alani, M.Sc. in Esthetic & Restorative Dentistry (Iraq). It highlights the successful non-surgical management of tooth #36 — a mandibular first molar previously restored with a zirconia crown, showing a large distal root lesion and severe apical curvature.
Keywords: root canal treatment lower molar, zirconia crown removal, severe apical curvature endodontics, large periapical lesion RCT, flexible NiTi files curved canals, hydraulic condensation obturation, ROGIN endodontic motor, apex locator endodontics, mandibular molar endodontics.

Dr. Othman H. Alani
Case Presentation
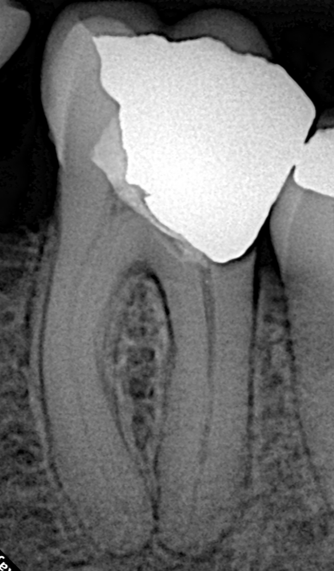
The patient was referred with a large radiolucent lesion surrounding the distal root of the crowned lower left first molar (#36). The periapical radiograph revealed substantial periapical pathology and pronounced curvature in the apical third of the root canal system. Such anatomy significantly increases the risk of procedural errors such as ledging, transportation, or instrument separation during shaping.
Diagnosis: Apical periodontitis with a massive distal root lesion.
Key Challenges:
- Removal of a full-coverage zirconia crown without compromising the remaining tooth structure.
- Assessing restorability after crown removal.
- Negotiating and shaping severely curved canals in the presence of infection.
- Achieving a predictable 3D seal in a complex canal system.
Treatment Plan
The primary goal was to remove the existing zirconia crown first to evaluate the underlying tooth structure and confirm restorability. If the tooth proved restorable, we would proceed with orthograde root canal treatment (RCT), including disinfection, shaping, and obturation, followed by a definitive composite restoration. Extraction would only be considered if the tooth was deemed non-restorable.
This conservative approach prioritizes tooth preservation in a molar that had already received a significant investment in a zirconia crown, in line with modern minimally invasive endodontic principles for teeth with large periapical lesions.

Clinical Procedure (Step-by-Step Workflow)
Step 1: Access and Crown Removal
The old zirconia crown was carefully sectioned and removed to assess the remaining coronal tooth structure. Restorability was confirmed, allowing progression to endodontic treatment. Zirconia crown removal requires controlled sectioning with appropriate diamond burs under water cooling to minimize heat and vibration while preserving dentin.
Step 2: Access Cavity and Orifice Flaring
After trepanation, the orifices were enlarged using the ROGIN Sx Orifice Opener. This created straight-line access, which is essential for negotiating curved canals and reducing stress on subsequent instruments.
Step 3: Working Length Determination
Working length (WL) was precisely determined using the ROGIN Apex_S apex locator. Electronic apex locators provide reliable readings even in wet or infected canals, offering greater accuracy than radiographic methods alone.
Step 4: Canal Shaping
Canal shaping was performed with the ROGIN Elite_Ino endo motor (a cordless brushless motor with integrated apex locator functionality). Due to the severe apical curvature, highly flexible instruments were essential to maintain the original canal anatomy and prevent iatrogenic errors.
Dr. Alani selected ROGIN Super Flexi Files — heat-treated NiTi rotary files known for their exceptional flexibility, high cutting efficiency, and resistance to cyclic fatigue. These files performed excellently in the curved and complex anatomies typical of mandibular molars, allowing safe navigation of the apical third without transportation or ledging.
Step 5: Obturation and Restoration
Obturation was completed using the hydraulic condensation technique, which leverages sealer hydraulics for excellent adaptation and a true 3D seal, particularly beneficial in irregular or curved canals. A final composite restoration sealed the access cavity, restoring both function and coronal integrity.


Clinical Tips for Similar Advanced Cases
- Flexibility is Key: ROGIN Super Flexi Files easily adapt to severe apical curvatures, effectively preventing ledges and canal transportation.
- Smart Equipment Synergy: The combination of ROGIN Apex_S (precision) and Elite_Ino Motor (stability) ensures excellent apical control in complex lesion cases.
- Assess First: Always remove old crowns to evaluate restorability before committing to root canal treatment.
- Straight-Line Access Matters: Adequate orifice flaring with dedicated openers greatly improves instrument control in posterior teeth with challenging anatomy.
- Hydraulic Condensation Advantages: This technique provides efficient filling with superior adaptation in complex canal morphologies while minimizing the risk of extrusion when performed properly.
Outcome and Takeaways
This case demonstrates that even advanced endodontic scenarios — involving zirconia crown removal, large periapical pathology, and severe root curvature — can be predictably managed non-surgically with careful planning, proper armamentarium, and meticulous technique. The tooth was successfully preserved, avoiding extraction and more invasive treatment options.
Dr. Othman H. Alani’s approach highlights the importance of early restorability assessment, respect for root canal anatomy, and the intelligent use of modern NiTi technology in achieving biological and functional success.