In endodontics, complex root canal anatomy continues to challenge even experienced clinicians. This advanced case from Ecuador highlights a successful conservative approach in a mandibular first molar presenting both a radix entomolaris and a middle mesial (MM) canal, while prioritizing the preservation of pericervical dentin for long-term biomechanical success.

Dr. Luis Coloma Calle demonstrates how meticulous diagnosis, proper negotiation, and a conservative mechanized system can effectively manage these anatomical variations.
Anatomical Variations in Mandibular First Molars
The mandibular first molar is one of the most commonly treated teeth in endodontics, yet it frequently presents unexpected complexities.
- Radix entomolaris: This additional distolingual root occurs in approximately 3% of cases, though the distolingual canal itself can be observed in up to 22% of mandibular molars depending on the population.
- Middle Mesial (MM) Canal: Located between the mesiobuccal and mesiolingual canals, its prevalence ranges from 1% to 15% according to CBCT and microscopic studies. One analyzed dataset reported a prevalence of approximately 5.09%, underscoring its clinical relevance despite being relatively uncommon.
These variations increase the risk of missed canals, inadequate disinfection, and procedural errors. Thorough knowledge and advanced visualization are essential for successful outcomes.

Clinical Challenges in This Advanced Case
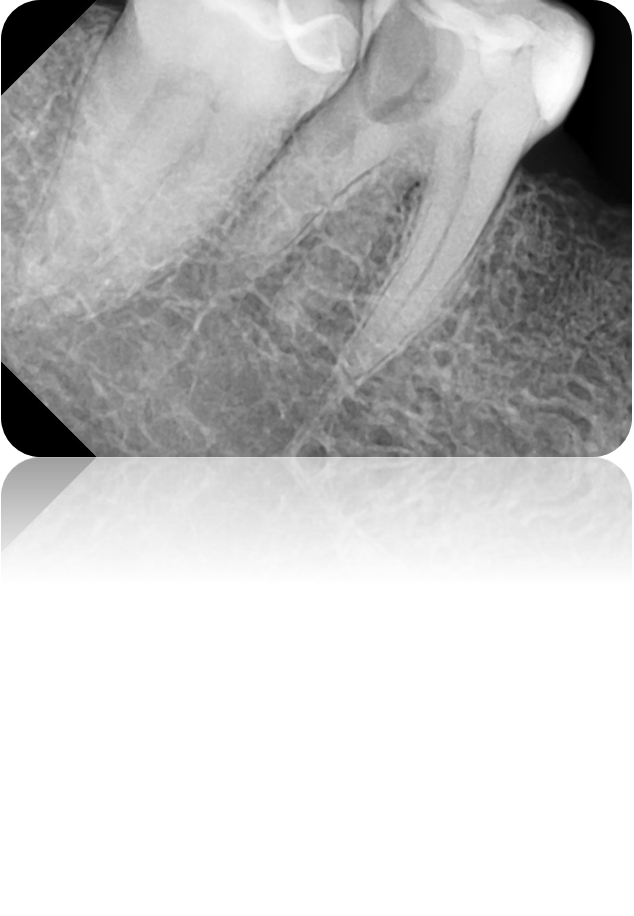
Tooth: Mandibular First Molar
Anatomy: Radix entomolaris + Middle Mesial (MM) canal
Main Challenge: High risk of ledging or instrument separation due to narrow, curved canals.
The presence of these accessory canals demands a precise and conservative strategy. Over-enlargement can compromise the pericervical dentin — the critical cervical zone of dentin that significantly contributes to the tooth’s fracture resistance.
Clinical Workflow and Treatment Protocol
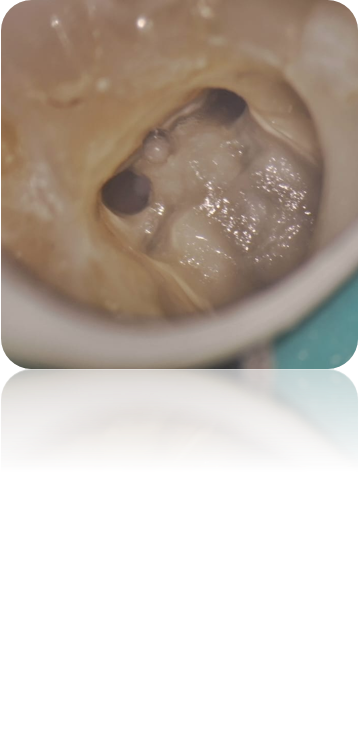
1. Localization of Canals
The middle mesial canal was identified through careful exploration of the groove connecting the mesiobuccal and mesiolingual orifices. This step was performed under dental operating microscope magnification combined with ultrasonics, which greatly enhances detection rates.
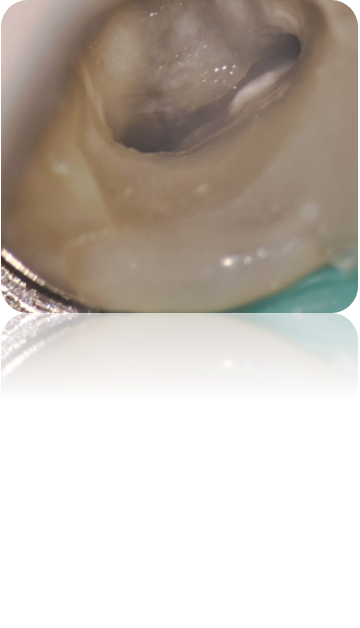
2. Negotiation
Once located, the middle mesial canal and radix entomolaris were carefully negotiated using small manual K-files (#08 and #10). These fine instruments allow safe initial scouting in narrow and curved anatomies without creating ledges or blockages.
3. Glide Path Establishment
A reliable glide path is fundamental for safe mechanized instrumentation. The R-Shaper 016 file from Rogin was used to create a smooth, predictable path, minimizing the risk of transportation or instrument fracture.
4. Shaping Phase
The case followed Plotino’s Triad for mechanized instrumentation:
- Negotiation
- Preflaring
- Glide Path establishment
These steps are essential before final shaping.
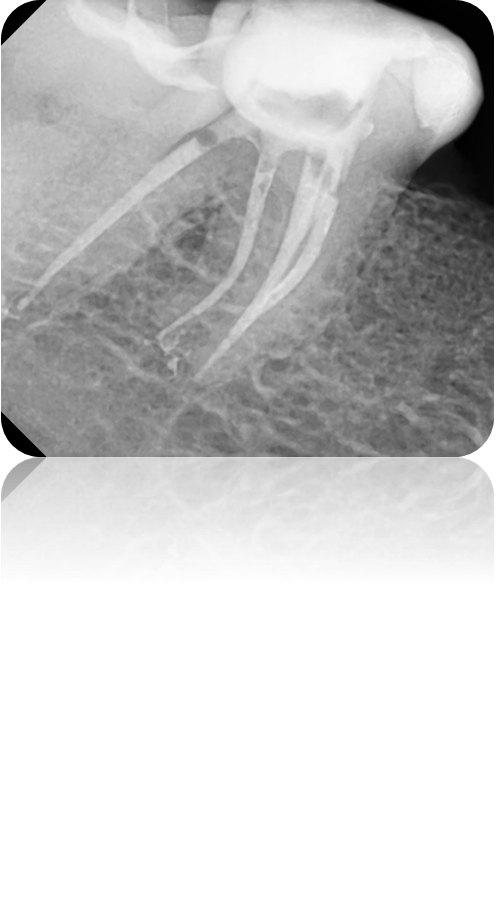
- Main canals were shaped up to R-Shaper S3 (30/.04).
- The radix entomolaris and middle mesial canal were prepared to R-Shaper S2 (25/.04).
The .04 taper of the R-Shaper system provided a conservative preparation that respected the original canal curvatures while achieving adequate cleaning and shaping without compromising pericervical dentin.
Clinical Tips for Managing Similar Cases
❗️ Protect Pericervical Dentin
Master Plotino’s Triad (Negotiate → Preflare → Glide Path) to maintain structural integrity and long-term prognosis.
❗️ Leverage Magnification
Always use a dental operating microscope to explore the mesial groove between MB and ML canals. This is the key to locating the middle mesial canal.
❗️ Choose Conservative Instruments
Systems with .04 taper like R-Shaper are excellent for complex anatomies, as they reduce the risk of over-enlargement while maintaining flexibility in curved canals.
❗️ Manual + Mechanical Synergy
Combine delicate manual negotiation with modern mechanized files for safer and more predictable results in high-risk cases.
Conclusion
This case exemplifies that anatomical complexity in mandibular first molars — including radix entomolaris and middle mesial canals — can be successfully managed through careful planning, advanced visualization, and conservative instrumentation protocols. By preserving pericervical dentin and strictly following proven sequences such as Plotino’s Triad, clinicians can achieve excellent cleaning, shaping, and long-term tooth survival.
Proper detection and treatment of these variants not only improve disinfection but also significantly reduce the risk of endodontic failure.